Yes, irs an excellent word and you used it in the proper context.This tells me how pussified(is that a word?) people are.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Covid Vaccine
- Thread starter jitter77
- Start date
@Confluence gonna love this article.
At Pfizer’s third-quarter earnings report teleconference on October 27, CEO Albert Bourla reported that the company had not reached the 32 cases required for the first interim analysis. This was disappointing news, given his earlier promises. The reality was that Pfizer was just shy. Two weeks later, on November 9th, Pfizer reported the massive success of their phase III trial with 94 cases, blowing past both the 32 and the 62 case interim timepoints. So what happened in those two weeks?
Somewhere between the end of October and the start of November, Pfizer voluntarily petitioned the FDA for a protocol change to ditch the 32-case interim analysis completely. While waiting for the FDA to approve this change, Science reported, “they decided to store the nasal swabs taken from participants who had suspected SARS-CoV-2 infections: If they didn’t test the swabs, they couldn’t confirm cases and therefore would avoid a protocol violation.” To put it in plain English: Those in charge at Pfizer decided they would rather not know the outcome of their clinical trial because they might have been legally required to disclose the results; as we now know, those results were so unequivocally positive that they sent the Dow Jones stock index soaring by nearly 3 percent the day they were finally disclosed.
Why would Pfizer rush to petition the FDA in the week before the election to change their clinical trial protocol and avoid the 32-case interim analysis? The stated rationale does not stand up to scrutiny. Ugur Sahin, the CEO of BioNTech, which co-developed the mRNA vaccine with Pfizer, offered the following explanation: “The math was simple: Covid-19 cases among participants were jumping from one or two per day to up to 10 or more. It became clear that the trial would accrue 62 cases shortly after hitting the 32 mark, and the higher number meant greater statistical power—and fewer debates about the meaning of the data. This 62 cutoff both lowered the efficacy bar the vaccine had to clear, and was also something of an insurance policy: If the vaccine triggered mediocre immune responses and it teetered around 50 percent efficacy in the trial, it could more easily have been deemed futile at 32 cases because of bad luck.”
At Pfizer’s third-quarter earnings report teleconference on October 27, CEO Albert Bourla reported that the company had not reached the 32 cases required for the first interim analysis. This was disappointing news, given his earlier promises. The reality was that Pfizer was just shy. Two weeks later, on November 9th, Pfizer reported the massive success of their phase III trial with 94 cases, blowing past both the 32 and the 62 case interim timepoints. So what happened in those two weeks?
Somewhere between the end of October and the start of November, Pfizer voluntarily petitioned the FDA for a protocol change to ditch the 32-case interim analysis completely. While waiting for the FDA to approve this change, Science reported, “they decided to store the nasal swabs taken from participants who had suspected SARS-CoV-2 infections: If they didn’t test the swabs, they couldn’t confirm cases and therefore would avoid a protocol violation.” To put it in plain English: Those in charge at Pfizer decided they would rather not know the outcome of their clinical trial because they might have been legally required to disclose the results; as we now know, those results were so unequivocally positive that they sent the Dow Jones stock index soaring by nearly 3 percent the day they were finally disclosed.
Why would Pfizer rush to petition the FDA in the week before the election to change their clinical trial protocol and avoid the 32-case interim analysis? The stated rationale does not stand up to scrutiny. Ugur Sahin, the CEO of BioNTech, which co-developed the mRNA vaccine with Pfizer, offered the following explanation: “The math was simple: Covid-19 cases among participants were jumping from one or two per day to up to 10 or more. It became clear that the trial would accrue 62 cases shortly after hitting the 32 mark, and the higher number meant greater statistical power—and fewer debates about the meaning of the data. This 62 cutoff both lowered the efficacy bar the vaccine had to clear, and was also something of an insurance policy: If the vaccine triggered mediocre immune responses and it teetered around 50 percent efficacy in the trial, it could more easily have been deemed futile at 32 cases because of bad luck.”
- Joined
- Apr 8, 2014
- Messages
- 12,661
- Reaction score
- 18,149
- Points
- 113
$100B in revenues, from taxpayers, because they rigged their data.@Confluence gonna love this article.
At Pfizer’s third-quarter earnings report teleconference on October 27, CEO Albert Bourla reported that the company had not reached the 32 cases required for the first interim analysis. This was disappointing news, given his earlier promises. The reality was that Pfizer was just shy. Two weeks later, on November 9th, Pfizer reported the massive success of their phase III trial with 94 cases, blowing past both the 32 and the 62 case interim timepoints. So what happened in those two weeks?
Somewhere between the end of October and the start of November, Pfizer voluntarily petitioned the FDA for a protocol change to ditch the 32-case interim analysis completely. While waiting for the FDA to approve this change, Science reported, “they decided to store the nasal swabs taken from participants who had suspected SARS-CoV-2 infections: If they didn’t test the swabs, they couldn’t confirm cases and therefore would avoid a protocol violation.” To put it in plain English: Those in charge at Pfizer decided they would rather not know the outcome of their clinical trial because they might have been legally required to disclose the results; as we now know, those results were so unequivocally positive that they sent the Dow Jones stock index soaring by nearly 3 percent the day they were finally disclosed.
Why would Pfizer rush to petition the FDA in the week before the election to change their clinical trial protocol and avoid the 32-case interim analysis? The stated rationale does not stand up to scrutiny. Ugur Sahin, the CEO of BioNTech, which co-developed the mRNA vaccine with Pfizer, offered the following explanation: “The math was simple: Covid-19 cases among participants were jumping from one or two per day to up to 10 or more. It became clear that the trial would accrue 62 cases shortly after hitting the 32 mark, and the higher number meant greater statistical power—and fewer debates about the meaning of the data. This 62 cutoff both lowered the efficacy bar the vaccine had to clear, and was also something of an insurance policy: If the vaccine triggered mediocre immune responses and it teetered around 50 percent efficacy in the trial, it could more easily have been deemed futile at 32 cases because of bad luck.”
All you need to understand is that Pfizer's safety and efficacy studies for the FDA shots are amazingly still not complete -- according to Pfizer-- and the terms have been so dramatically amended so as to leave them useless.
Just as the story above indicates, they rigged the studies for $100B.
fraud
/frôd/
noun
wrongful or criminal deception intended to result in financial or personal gain.
All I see is that Pfizer thinks it can continue to milk this cow.


- Joined
- Apr 8, 2014
- Messages
- 12,661
- Reaction score
- 18,149
- Points
- 113
Moving the goalposts, with help from Fauci:
Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available. Surprisingly, little has changed with influenza vaccines since 1957 when they were first administered in US national vaccination programs. Over the years, influenza vaccines have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains.
Although current influenza vaccines reduce the risk of severe disease, hospitalization, and death to some degree, their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.
Furthermore, the duration of vaccine-elicited immunity is measured only in months. Current vaccines require annual re-vaccination with updated formulations that are frequently not precisely matched to circulating virus strains.
Although annual influenza vaccinations are strongly recommended for most of the general public and especially for persons in high-risk groups, including the elderly, those with chronic diseases, and pregnant women, vaccine acceptance by the general public is not ideal.
As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.
Even decades-long efforts to develop better, so-called “universal” influenza vaccines—vaccines that would create more broadly protective immunity, preferably lasting over longer time periods—have not yet resulted in next-generation, broadly protective vaccines, although a large number of experimental vaccines are in preclinical or early clinical development.
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure, including candidate vaccines against RSV, a major killer of infants and the elderly, parainfluenzaviruses, endemic coronaviruses, and many other “common cold” viruses that cause significant morbidity and economic loss.
More than 50 years ago, the development of successful vaccines against some of the most important respiratory viruses, including measles, mumps, and rubella, led to the hope that vaccines could soon be developed for all other respiratory viruses. However, natural infections with these three vaccine-controlled respiratory viruses, as well as smallpox and varicella zoster virus (VZV), are not representative of infections caused by most respiratory viruses. They differ in at least three critically important ways that are related to their successful control with vaccines (Table 1):
Here is the link for more:
There are some more nuggets:
Rapid antigenic drift affects the control of annual influenza epidemics and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity that has complicated its control through current vaccination strategies.
Summary
Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other “common cold” viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines. In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled. We discuss possible approaches to developing next-generation vaccines against these viruses, in consideration of several variables such as vaccine antigen configuration, dose and adjuventation, route and timing of vaccination, vaccine boosting, adjunctive therapies, and options for public health vaccination polices.Introduction
Effective vaccines and vaccine prevention strategies against endemic and emerging respiratory viruses are of critical importance, as these pathogens kill as many as 5 million people worldwide every year. For example, over the past decade, influenza killed 12,000–52,000 people in the United States each year and ranks among the leading causes of years of productive life lost (YPLL). Endemic respiratory viruses such as respiratory syncytial virus (RSV) and the parainfluenzaviruses take many additional lives, and previously unrecognized respiratory viruses such as SARS-CoV-2, the cause of COVID-19, have emerged unexpectedly. SARS-CoV-2 thus far has killed more than one million people in the United States. The increasing frequency of emergences of such pandemic respiratory viruses may be a key feature of a new pandemic era, forcing us to consider anew the state of respiratory virus vaccinology (Figure 1) .Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available. Surprisingly, little has changed with influenza vaccines since 1957 when they were first administered in US national vaccination programs. Over the years, influenza vaccines have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains.
Although current influenza vaccines reduce the risk of severe disease, hospitalization, and death to some degree, their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.
Furthermore, the duration of vaccine-elicited immunity is measured only in months. Current vaccines require annual re-vaccination with updated formulations that are frequently not precisely matched to circulating virus strains.
Although annual influenza vaccinations are strongly recommended for most of the general public and especially for persons in high-risk groups, including the elderly, those with chronic diseases, and pregnant women, vaccine acceptance by the general public is not ideal.
As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.
Even decades-long efforts to develop better, so-called “universal” influenza vaccines—vaccines that would create more broadly protective immunity, preferably lasting over longer time periods—have not yet resulted in next-generation, broadly protective vaccines, although a large number of experimental vaccines are in preclinical or early clinical development.
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure, including candidate vaccines against RSV, a major killer of infants and the elderly, parainfluenzaviruses, endemic coronaviruses, and many other “common cold” viruses that cause significant morbidity and economic loss.
More than 50 years ago, the development of successful vaccines against some of the most important respiratory viruses, including measles, mumps, and rubella, led to the hope that vaccines could soon be developed for all other respiratory viruses. However, natural infections with these three vaccine-controlled respiratory viruses, as well as smallpox and varicella zoster virus (VZV), are not representative of infections caused by most respiratory viruses. They differ in at least three critically important ways that are related to their successful control with vaccines (Table 1):
- (1) after first replicating mucosally, these systemic respiratory viruses all cause significant viremia that seeds an enormous number of infectious virions throughout the body, putting them in contact with multiple immune compartments and immune competent cell types,
- (2) they have relatively long incubation periods that reflect initial mucosal replication and the subsequent systemic spread of infectious virions, which allows time for the induction of the full force of adaptive immunity, and
- (3) they elicit long-term or lifetime protective immunity (Table 1).
Here is the link for more:
There are some more nuggets:
Rapid antigenic drift affects the control of annual influenza epidemics and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity that has complicated its control through current vaccination strategies.
- Joined
- Apr 8, 2014
- Messages
- 12,661
- Reaction score
- 18,149
- Points
- 113
The Fauci paper actually, categorically shows that influenza shots do not work, because they cannot:
Table 1
Epidemiologic and immunologic parameters of selected human respiratory viruses and vaccines used to control them
Table 1
Epidemiologic and immunologic parameters of selected human respiratory viruses and vaccines used to control them
| Virus | Incubation period a | Marked viremia | Infection elicits long-term protective immunity | Re-infections are rare | Vaccines elicit long-term protective immunity | Vaccine type |
|---|---|---|---|---|---|---|
| Measles (to prodrome) | ≈10 days | yes | yes | yes | yes | replicating |
| Mumps | ≈16 days | yes | yes | yes | yes | replicating |
| Rubella | ≈16 days | yes | yes | yes | yes | replicating |
| Smallpox b | ≈12 days | yes | yes | yes | yes | replicating |
| VZV c | ≈14 days | yes | yes | yes | yes | replicating |
| Endemic coronaviruses | ≈5 days | no | no | no | no | none |
| Influenza virus | ≈2 days | no | no | no | no | replicating, other |
| Parainfluenzaviruses | ≈4 days | no | no | no | no | none |
| RSV | ≈5 days | no | no | no | no | none |
Hammering that Cochrane study. Great opinion piece by a Levi Strauss brand president, and the sheep he had to endure.
Masks...don't work.
As he says....I'm pro-science because I am anti-mask.
Masks...don't work.
As he says....I'm pro-science because I am anti-mask.
Sweet little article for the upcoming Covid commission. Top ten questions that should be asked by said commission.
1. What Could Have Been Done to Better Protect Older, High-Risk Americans?
2. Why Was Natural Immunity to Covid Ignored?
3. Why Were Schools and Colleges Closed?
4. Why Was Covid Prioritized over Other Health Problems?
5. Why Did the CDC Fail to Collect Accurate Data About the Virus?
6. Why Did Public Health Officials Trust Unreliable Models?
7. Why Was There a Concentrated Effort to Demonize Potential Covid Therapeutics?
8. Why Did Public Health Officials Disregard Safety Protocols for the Covid Jabs?
9. How Did the U.S. Get Its Covid Testing Policies So Wrong?
10. Why the Massive Push for Ineffective Mask Mandates?
Hmmmm. True?
Update on the unusually high trend of athletes dying - that the NIH acknowledges.
A study by Maron on sudden death in US athletes, from 1980 to 2006 in thirty-eight sports identified 1,866 deaths of athletes with cardiac disease, with a prevalence of hypertrophic cardiomyopathy.
2005 to 2006 averaged sixty-six (66) deaths per year, with 82% of those occurring during competition or training.
Thanks to investigator readers for discovering these reports, and this story in Spanish: Momento Deportivo.
In 2021 and 2022 so far, cardiac disease has not been mentioned. Hypertrophic cardiomyopathy was mentioned twice, but those two reports were listed in the “not vax related” list. “Enlarged heart” was only mentioned three times, but there was no indication this was a long-term or recent issue (possibly due to vaccine injury).
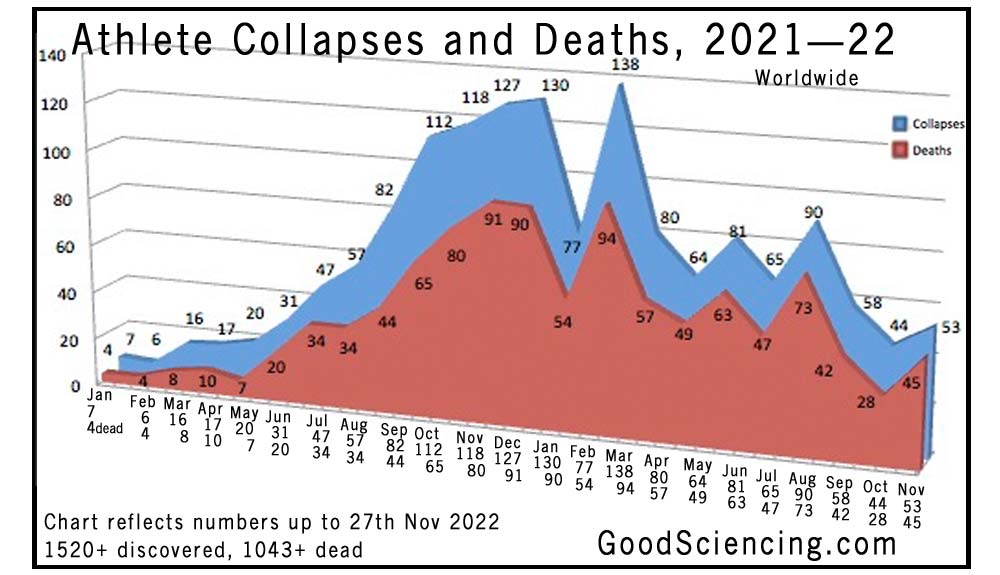
The above shows that in prior years, there were 66 deaths per year, but there have been 89 reported in January 2022, so far.

Athlete collapses and deaths chart from 1st January 2021 to 31st December 2022. Good Sciencing.
New Note: The number of new cancers appear to be increasing. In other places, we have seen doctors reporting that there are 5 times more cancers and many of those go straight to stage 4. We draw no conclusions from this, but the small list we are working on contains several newly-discovered cancer deaths.
List of January deaths on the next page
1520 Athlete Cardiac Arrests, Serious Issues, 1043 of Them Dead, Since COVID Injection - Real Science
It is not normal for young athletes to suffer cardiac arrest or death while playing sport, but most of these come shortly after a COVID shot.
goodsciencing.com
Prior Year Data
The International Olympic Committee in Lausanne, Switzerland, studied documents from international data banks from 1966 to 2004. Those documents indicate 1,101 sudden deaths in athletes under 35 years of age, an average of 29 athletes per year, the sports with the highest incidence being soccer and basketball. (NIH Document)A study by Maron on sudden death in US athletes, from 1980 to 2006 in thirty-eight sports identified 1,866 deaths of athletes with cardiac disease, with a prevalence of hypertrophic cardiomyopathy.
2005 to 2006 averaged sixty-six (66) deaths per year, with 82% of those occurring during competition or training.
Thanks to investigator readers for discovering these reports, and this story in Spanish: Momento Deportivo.
In 2021 and 2022 so far, cardiac disease has not been mentioned. Hypertrophic cardiomyopathy was mentioned twice, but those two reports were listed in the “not vax related” list. “Enlarged heart” was only mentioned three times, but there was no indication this was a long-term or recent issue (possibly due to vaccine injury).
The above shows that in prior years, there were 66 deaths per year, but there have been 89 reported in January 2022, so far.
Athlete collapses and deaths chart from 1st January 2021 to 31st December 2022. Good Sciencing.
New Note: The number of new cancers appear to be increasing. In other places, we have seen doctors reporting that there are 5 times more cancers and many of those go straight to stage 4. We draw no conclusions from this, but the small list we are working on contains several newly-discovered cancer deaths.
List of January deaths on the next page







- Joined
- Apr 8, 2014
- Messages
- 8,664
- Reaction score
- 9,182
- Points
- 113
Many of these people have no cause or even circumstances of death listed, some of them are well over 35, some of them aren't dead, at least a couple of them (Lemonier and Dunn) are rumored to have committed suicide, you've got aneurysms cancer, bacterial infection, amputation, Ons Jabeur "collapsing" in tears after a grueling 3 set match with a knee injury at 1 a.m. at the end of a long tournament...and you're listing them all as "data" to compare to numbers of sudden deaths in athletes under 35.Continued....one month of data only. We're not joking when we say it happens every day.
View attachment 10484
View attachment 10485
View attachment 10486
View attachment 10487
View attachment 10488
View attachment 10489
View attachment 10490
This "data" is a list of people of varying ages who became ill to varying degrees from various causes and/or died from various causes, some of them unknown to the public.
"Good Sciencing" lol.
Last edited:
- Joined
- Apr 8, 2014
- Messages
- 8,664
- Reaction score
- 9,182
- Points
- 113
Not only that, but
Huh, the 66 number was a study of young US competitive athletes who died suddenly ranged in age from 8 to 39, and the list of 89 reported in January (many of whom we've already established aren't even actually dead) are people from all over the globe and range up to the age of 72.The above shows that in prior years, there were 66 deaths per year, but there have been 89 reported in January 2022, so far.
Many of these people have no cause or even circumstances of death listed, some of them are well over 35, some of them aren't dead, at least a couple of them (Lemonier and Dunn) are rumored to have committed suicide, you've got aneurysms cancer, bacterial infection, amputation, Ons Jabeur "collapsing" in tears after a grueling 3 set match with a knee injury at 1 a.m. at the end of a long tournament...and you're listing them all as "data" to compare to numbers of sudden deaths in athletes under 35.
This "data" is a list of people of varying ages who became ill to varying degrees from various causes and/or died from various causes, some of them unknown to the public.
"Good Sciencing" lol.
The cancers are explained in a prior post. Many suspect the spike proteins are causing cancers. People who've been in remission for years all of a sudden having stage 4 cancer. Studies should ensue.
You can go case by case and suggest anomalies. What you cannot do is ignore the absolute numbers. More athletes are dying by a greater percentage than ever before. By quite a lot. The National Institutes of Health admits as such.
Why? I'm sure it's all very rational and has nothing at all to do with the vaccines that attack human hearts.
Not only that, but
Huh, the 66 number was a study of young US competitive athletes who died suddenly ranged in age from 8 to 39, and the list of 89 reported in January (many of whom we've already established aren't even actually dead) are people from all over the globe and range up to the age of 72.
From the article, which you apparently missed.
Important Notes: The number of dead are included in the total number. There are also dozens of reports that are not included in the total number shown in the headline because they are not or may not be vaccine-related, in our judgement.
In response to their pronouncement, here is a non-exhaustive and continuously growing list of mainly young athletes who had major medical issues in 2021/2022 after receiving one or more COVID vaccines.
They say clearly not all are deaths. The chart even delineates between collapses and deaths.
The International Olympic Committee in Lausanne, Switzerland, studied documents from international data banks from 1966 to 2004. Those documents indicate 1,101 sudden deaths in athletes under 35 years of age, an average of 29 athletes per year, the sports with the highest incidence being soccer and basketball. (NIH Document)
A study by Maron on sudden death in US athletes, from 1980 to 2006 in thirty-eight sports identified 1,866 deaths of athletes with cardiac disease, with a prevalence of hypertrophic cardiomyopathy.
2005 to 2006 averaged sixty-six (66) deaths per year, with 82% of those occurring during competition or training.
The Maron study focused on those 39 and under. 1,866 deaths from 1980 to 2006. Give or take the average was 66 per YEAR.
With those over 39 included, there were 63 deaths in November alone. A month.
Take out those over 39 if you want. Athletes are in fact dying at higher rates than ever before.
- Joined
- Apr 8, 2014
- Messages
- 8,664
- Reaction score
- 9,182
- Points
- 113
What is the study that produced the data from "the chart"? Because the chart certainly has no relationship whatsoever in terminology or methodology to the two studies you posted. What qualifies as a "collapse"? Is that a medical term? Or are these just random stories people found on the internet and put into a chart? The Ons Jabeur "collapse" is in the same category as the Damar Hamlin "collapse"?From the article, which you apparently missed.
They say clearly not all are deaths. The chart even delineates between collapses and deaths.
The Maron study focused on those 39 and under. 1,866 deaths from 1980 to 2006. Give or take the average was 66 per YEAR.
With those over 39 included, there were 63 deaths in November alone. A month.
Take out those over 39 if you want. Athletes are in fact dying at higher rates than ever before.
Please post a study which shows "athletes are dying at higher rates than ever before".
- Joined
- Apr 8, 2014
- Messages
- 8,664
- Reaction score
- 9,182
- Points
- 113
66 deaths of YOUNG US athletes per year. Your "data" includes people from all over the world. And includes people who didn't die. And includes people who weren't ever even in danger of dying, And includes people who are not young. Not to mention that we don't even have any idea if any of them were even vaccinated but that's another argument.The Maron study focused on those 39 and under. 1,866 deaths from 1980 to 2006. Give or take the average was 66 per YEAR.
US population 331 million.
World population 7.9 billion.
So yes, the number of athletes who die (or collapse, or get cancer, or get bacterial infections, or fall to their knees and cry after losing a tennis match) all over the world is going to be considerably larger than the number of young US athletes who die.
You are comparing apples to bicycles.
Oh ****are over 50, a fat ***, or generally just paranoid, you should be very, very afraid, because it's still out there and coming for you.
- Joined
- Apr 8, 2014
- Messages
- 12,661
- Reaction score
- 18,149
- Points
- 113
OFTB is adopting the Flogtard posting strategy.
- Joined
- Sep 12, 2014
- Messages
- 18,110
- Reaction score
- 7,003
- Points
- 113
I totally support the current thing.
It's so important, I wish more people could understand and appreciate how important the current thing is to all of us.
I read somewhere, sorry can't find the link, that the CDC is now adding an annual Covid booster to their list of recommended vaccines.
I suppose those that subscribe to my first statement will quickly fall in line, but it's just a little too hinky (medical term, known only to Dokters) for me.
It's so important, I wish more people could understand and appreciate how important the current thing is to all of us.
I read somewhere, sorry can't find the link, that the CDC is now adding an annual Covid booster to their list of recommended vaccines.
I suppose those that subscribe to my first statement will quickly fall in line, but it's just a little too hinky (medical term, known only to Dokters) for me.
- Joined
- Sep 12, 2014
- Messages
- 18,110
- Reaction score
- 7,003
- Points
- 113
Much like “Athlete Collapses and Deaths”.I totally support the current thing.
It's so important, I wish more people could understand and appreciate how important the current thing is to all of us.
I read somewhere, sorry can't find the link, that the CDC is now adding an annual Covid booster to their list of recommended vaccines.
I suppose those that subscribe to my first statement will quickly fall in line, but it's just a little too hinky (medical term, known only to Dokters) for me.